“I Saw an Ad for a Much Cheaper Option. Is It the Same Thing?”
“We found a clinic offering something called sermorelin for a fraction of the price. Is it just as good as growth hormone?”
“I read online about peptides as an alternative. What’s the difference? If growth hormone peptides too?”
These questions come up more and more in our consultations, and I understand why. If you have been researching growth hormone online, you have almost certainly seen advertisements from medical spas and wellness clinics promoting peptide-based therapies at a significantly lower price point. The marketing is polished, the claims sound compelling, and the cost comparison alone is enough to make any parent pause.
But before your family makes a decision based on what you have seen online, there is a fundamental distinction you deserve to understand clearly. It is not a matter of preference or opinion. It is a matter of science, regulatory approval, and your child’s one and only opportunity to grow.
I’m Jenny Diep, FNP at I Grow Clinic. Let me walk you through exactly what the evidence says.
Why Families Trust I Grow Clinic
| Clinic Standard | What It Means for Your Family |
|---|---|
| Nearly 3,000 children guided | Proven experience with real-world growth decisions |
| 95% treatment retention | Families stay because outcomes match expectations |
| AI-driven bone age analysis | Every treatment decision backed by precision data |
| Board-certified Medical Director, 20+ years | Expert oversight at every step |
| Telehealth in CA, NY, TX, WA, FL | Specialist access regardless of where you live |
| 5-Star Google Rating | Trust built through transparency and results |

First: What Even Is a Peptide?
The word “peptide” simply refers to a chain of amino acids. By that definition, human growth hormone is technically a peptide, which is a fact that gets used heavily in marketing to blur the line between very different categories of medicine.
But calling everything a “peptide” is like calling both a tricycle and a commercial aircraft “vehicles.” The word is technically accurate, but it tells you almost nothing useful about how they work, what they are capable of, or whether one is safe to board with your child.
The compounds being sold at medical spas and wellness clinics as “growth hormone peptides” or “HGH peptides” are not growth hormone. They belong to a class of short synthetic compounds called growth hormone releasing peptides (GHRPs) or growth hormone releasing hormone analogs (GHRHs). Names you may have seen include sermorelin, CJC-1295, GHRP-2, GHRP-6, hexarelin, and ipamorelin, among others.
These compounds do not deliver growth hormone to the body. They attempt to signal the pituitary gland to produce and release more of its own growth hormone. That is a fundamentally different mechanism, and in children, the distinction has real consequences.
🔍 To understand how growth hormone works in the body and what it does for growing children, read: Why I Started a Growth Hormone Clinic
How Real Growth Hormone Works
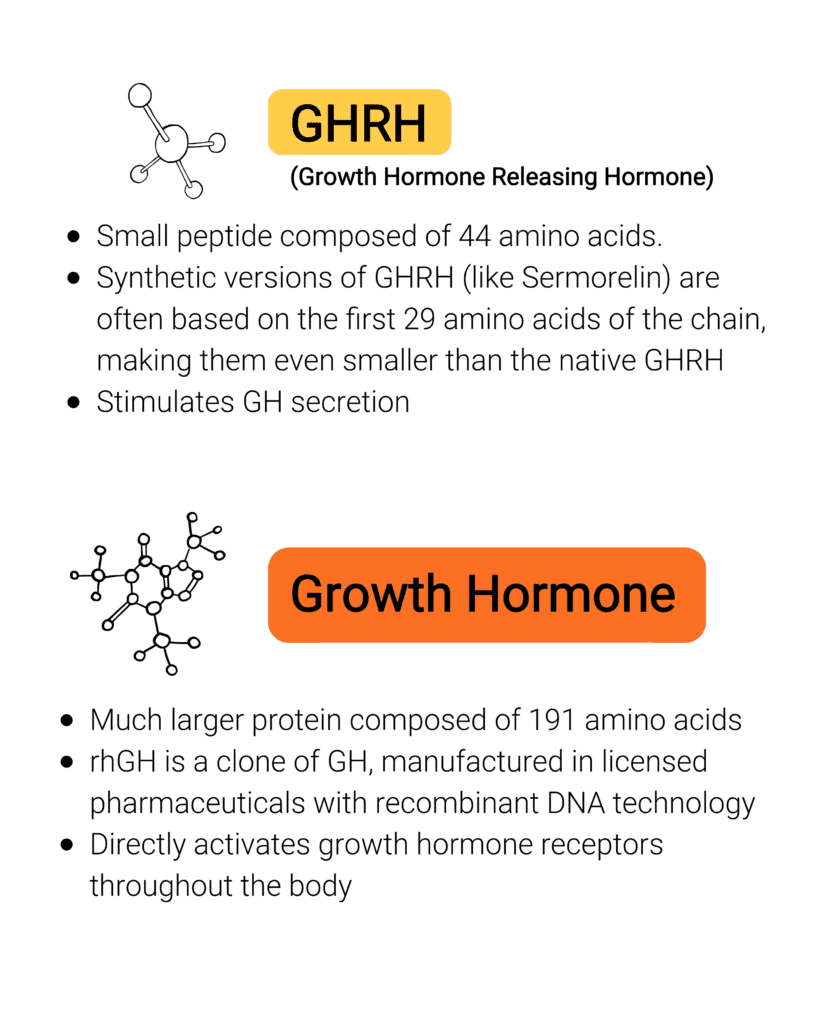
Pharmaceutical-grade recombinant human growth hormone (rhGH) is a bioidentical molecule. It is a precise replica of the 191 amino acid protein your child’s pituitary gland naturally produces. When administered, it binds directly to growth hormone receptors throughout the body and triggers a predictable, measurable cascade of effects, most importantly a sustained rise in IGF-1, the key driver of bone lengthening and linear height growth.
This is why rhGH has been the established standard of care in pediatric growth medicine for nearly 50 years since its FDA approval in 1985. The dosing is standardized, the monitoring protocols are well defined, and the long-term outcomes including final adult height data are extensively documented in large international registries involving hundreds of thousands of children.
rhGH vs. Peptides: What the Evidence Actually Shows
| Feature | FDA-Approved rhGH | Growth Hormone Peptides |
|---|---|---|
| Delivers actual growth hormone | Yes | No |
| FDA-approved for children | Yes | No |
| Sustained IGF-1 elevation | Yes | Not reliably |
| Proven final adult height gain | Yes | No consistent evidence |
| Long-term pediatric safety data | Decades | Essentially none |
| Manufactured by | Licensed pharmaceutical company | Compound pharmacy |
| Standardized dosing and monitoring | Yes | No |
How Peptides Work Differently
Peptides like sermorelin or CJC-1295 do not deliver growth hormone. They nudge the pituitary to release a pulse of its own growth hormone. The key problem with this approach in children is that the response is indirect, brief, and highly variable.
Studies on GHRPs in children showed some short-term increases in growth velocity, but there are critical limitations that are rarely mentioned in marketing materials.
IGF-1 levels did not rise sustainably. IGF-1 is the primary biomarker we use to confirm that growth hormone is actually working at the tissue level. GHRP studies consistently failed to demonstrate the kind of sustained IGF-1 elevation that rhGH produces. Without that sustained signal, bone lengthening is unreliable.
Responses varied widely between patients. Unlike rhGH, where dosing can be precisely calibrated to body weight and monitored through standardized lab values, peptide responses are inconsistent. Some children respond, others do not, and there is no reliable way to predict or control the outcome.
No evidence of improved final adult height. Short-term increases in growth velocity are not the same as lasting height gain. None of the available pediatric peptide studies demonstrated improvement in final adult height, which is the only outcome that truly matters for a growing child.
🔍 To understand why IGF-1 levels are such a critical marker of treatment effectiveness, read: IGF-1 Levels and Height Growth (Coming soon)
The Safety Question: What We Know and What We Don’t
rhGH (human growth hormone) has been used in millions of children over nearly five decades. Large international safety registries have tracked patients for years, and the known risks are well characterized, rare, and closely monitored. When prescribed and managed appropriately, the long-term safety profile is well understood.
Peptides, by contrast, have essentially no long-term pediatric safety data. The available studies are short, lasting only six to eight months in most cases, and they were not designed to track the outcomes that matter most for a growing child: effects on growth plate progression, impact on puberty timing, long-term metabolic consequences, and cancer risk over time.
This is not a minor gap. Growth hormone and peptides both work through the same GH-IGF-1 pathway. That means that whatever long-term risks exist for one, theoretically exist for the other. But while we have decades of monitoring data on rhGH, we have almost nothing for peptides in children. In pediatric medicine, “we don’t know yet” is not reassurance. It is a reason for caution.
Why Peptides Are Cheaper, and Why That Is Not a Good Sign
Real, pharmaceutical-grade human growth hormone is a large, complex 191 amino acid molecule. Producing it correctly requires sophisticated biotechnology, strict manufacturing standards, rigorous batch testing, and continuous regulatory oversight. It cannot be replicated in a compounding pharmacy. Every vial of legitimate rhGH is produced by a licensed pharmaceutical manufacturer and subject to the same quality controls as any other FDA-approved biologic.
Peptides are shorter, simpler molecules. They can be compounded in a pharmacy, which is precisely what most medical spas and wellness clinics are doing. Compounded preparations are not subject to the same pre-approval safety and efficacy testing required for FDA-approved biologics. Batch-to-batch consistency cannot be assured. Contamination risks, variable potency, and inconsistent dosing are real concerns that have been documented in the literature.
The lower price tag does not mean a better deal. It means a different product, produced under different standards, with different evidence, for a different patient population than your child.
🔍 For more on what growth hormone cost and access actually look like for families, read: Growth Hormone Cost and Insurance Coverage
What About Sermorelin Specifically?
Sermorelin is one of the most commonly marketed peptides and deserves specific mention because its history is often cited to imply legitimacy.
Sermorelin did receive limited FDA approval in the past, but not for the reasons it is currently being marketed. It was approved specifically for diagnosing growth hormone deficiency, not for treating idiopathic short stature or general height enhancement in healthy children. The approval was later withdrawn. Today, sermorelin is compounded and dispensed outside the FDA-approved framework, meaning it carries none of the regulatory protections that come with an approved drug.
Early studies in the 1980s and 1990s did show that sermorelin could increase growth velocity in certain children over short periods. But those studies were brief, the responses were variable, and no study has demonstrated improvement in final adult height. The evidence that was once considered promising has not held up to the standards that modern pediatric medicine requires.
Why We Don’t Use Peptides at I Grow Clinic
Our position is simple and grounded entirely in evidence.
rhGH is the established, FDA-approved standard of care for children with growth concerns. It has decades of efficacy and safety data. The dosing is precise, the monitoring is well defined, and the outcomes are documented. When we treat a child at I Grow Clinic, we can track IGF-1 levels, monitor bone age progression, adjust the dose based on response, and make decisions anchored in data that has been validated over generations of pediatric patients.
Peptides offer none of that. The evidence for efficacy in children is weak and short-term. The safety data is essentially nonexistent for long-term use. The manufacturing standards are lower. And most importantly, children only have one growth window. We are not willing to spend part of that window on a treatment that may not work reliably, that cannot be properly monitored, and whose long-term effects we cannot confidently predict.
The marketing is convincing and the medical landscape is genuinely confusing. But we do make it our responsibility to explain the difference clearly, so that every family we work with can make a truly informed decision.
A Note to Parents Who Are Weighing Their Options
Peptides are not the same as growth hormone. They are not a natural version of the same thing. They are a different class of compound, used in a different patient population, under different regulatory standards, with a fundamentally weaker evidence base when it comes to growing children.
Your child deserves the real medicine. And they deserve a team that will monitor it carefully, adjust it precisely, and stand behind it with data.
Whether you are in Southern California or connecting with us via telehealth from New York, Texas, Washington, or Florida, we are here to give your family the clarity it deserves.
FAQ: What Parents Ask About Peptides vs. Growth Hormone
1. Is sermorelin safe for children?
Sermorelin was once used in limited clinical settings for growth hormone deficiency diagnosis, but it is not FDA-approved for treating short stature in children. Today it is compounded outside the approved framework, and long-term safety data in children is essentially nonexistent. We do not recommend it as an alternative to rhGH for pediatric growth.
2. If peptides can increase growth hormone levels, why aren’t they used for kids?
Because increasing growth hormone levels briefly and unpredictably is not the same as producing the sustained, measurable IGF-1 elevation that drives consistent bone lengthening. Peptide studies in children failed to show sustained IGF-1 rises or improvement in final adult height, which is the standard we hold any treatment to.
3. My child’s doctor mentioned peptides as a possibility. Should I be concerned?
Peptides are increasingly used in adult wellness settings, and some physicians may mention them in passing. For children specifically, the evidence base does not support their use as a substitute for rhGH. We recommend consulting with a specialist who focuses on pediatric growth before making any decisions.
4. Can peptides be combined with real growth hormone?
There is no established evidence-based protocol for combining peptides with rhGH in children. At our clinic, we do not use this combination, and we would not recommend pursuing it outside of a formal clinical trial setting.
5. Are there any peptides that are actually FDA-approved for children?
No growth hormone releasing peptide is currently FDA-approved for height promotion in children, including those with idiopathic short stature. Some peptides have approvals for other conditions in adults, but none of those approvals extend to pediatric short stature.
Explore More
Why I Started a Growth Hormone Clinic
Bone Age vs. Chronological Age: Is Your Child’s Biological Clock Ticking Too Fast?
Growth Hormone Cost and Insurance Coverage: What U.S. Parents Need to Know