The X-Ray Results Are In. Now What?
“The radiologist said her bone age is two years ahead. What does that even mean for her height?”
“The doctor ordered a bone age X-ray for my son. We got the report back and it says something about “epiphyseal plates” and “skeletal maturity.” I have no idea how to read this, and no one explained it to us.”
If either of these moments sounds familiar, you are not alone. A bone age X-ray report can feel like reading a foreign language, especially when the stakes feel this high. The numbers on that page are not just data points. They represent a window of time that is either still open for your child or quietly narrowing, and understanding what the report is telling you is the first step toward using that information wisely.
The truth is that most radiology reports are written for physicians, not for parents. They use clinical shorthand that assumes years of medical training. But the underlying biology is not actually complicated, and once you understand what growth plate maturity really means and how to connect it to your child’s height future, you will be able to have a far more productive conversation with any provider you see.
A Note from Jenny Diep, FNP at I Grow Clinic
I am Jenny Diep, a Family Nurse Practitioner at I Grow Clinic in Fullerton, California. I work with families every week who are navigating exactly this kind of confusion. We have guided more than 2,500 children through their unique growth journeys, and the most common gap we see is this: parents receive a bone age result but have no framework for understanding what it means for their child specifically.
That is why I am writing this guide to equip you. Whether your child’s bone age is ahead, behind, or perfectly matched to their calendar age, knowing how to interpret that information is one of the most powerful things you can do as a parent.
Why Families Trust I Grow Clinic
| Patients Guided | Over 2,500 children with precision growth strategies |
| Retention Rate | 95% treatment retention rate |
| Care Model | Meticulous 1:1 personalized management with AI-driven bone age analysis |
| Medical Director | Dr. Choi, Board Certified by ABPMR, 20+ years of experience |
| Rating | 5-Star Google Rating with numerous family testimonials |
| Telehealth | Available in CA, NY, WA, FL, and TX |
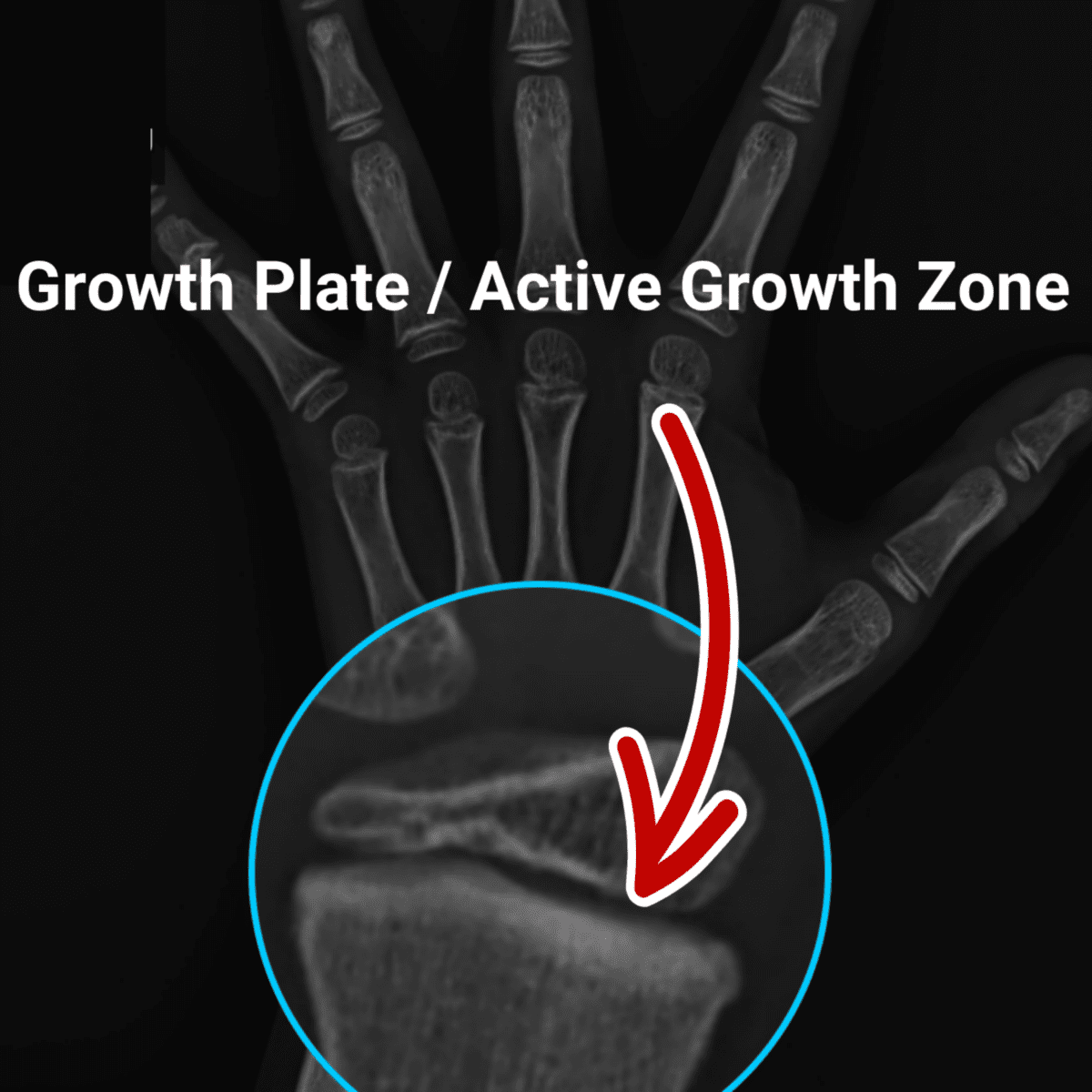
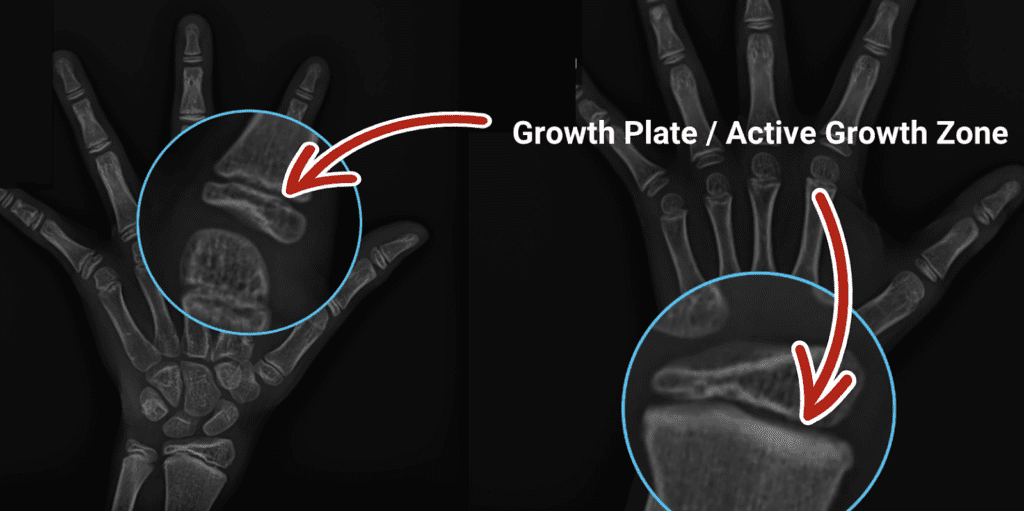
What Is a Growth Plate X-Ray, Bone age study and Why the Hand?
Before we can interpret the results, it helps to understand what is actually being measured.
A bone age study, also called a skeletal age X-ray, uses a single view, one low-dose X-ray of the left hand and wrist. This takes about two to three minutes from start to finish and involves only a very small amount of radiation, far less than a dental X-ray. The child simply places their left hand flat on the imaging surface, and the image is captured.
So why the hand specifically? The hand and wrist contain a remarkable number of small bones, 27 in total, along with multiple growth plates that mature in a highly predictable, well-documented sequence. Because of this consistent pattern, a single image of the hand allows a trained clinician to estimate the biological maturity of the entire skeletal system. It acts as a representative sample of what is happening in the long bones of the legs and arms, and even in the spine and pelvis.
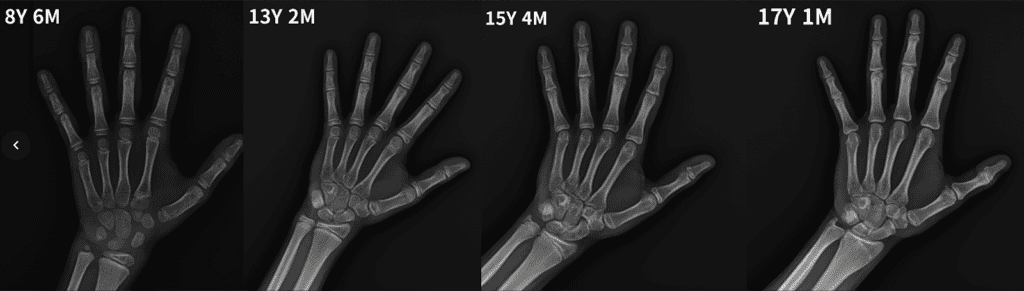
The two most widely used reference systems for interpreting these images are the Greulich-Pyle (GP) atlas, which compares your child’s X-ray against a standardized library of images, and the Tanner-Whitehouse method, which scores the maturity of individual bones for a more granular result. Both methods rely on a trained human eye comparing one image against a reference set, which means the result is only as precise as the reader’s experience and attention in that moment. A radiologist reviewing dozens of studies in a single day may catch the most obvious findings, but the subtle, early-stage changes in individual growth plates can be easy to miss.
At I Grow Clinic, we take this analysis a significant step further with AI-enhanced bone age assessment. Unlike traditional interpretation, our AI evaluates every single growth plate in the image, not just the most prominent ones, cross-referencing each against thousands of data points with microscopic precision. This level of systematic analysis is simply not feasible for the human eye to replicate consistently. The result is a bone age estimate that is measurably more accurate, more reproducible, and far less dependent on any single reader’s judgment. For families making important decisions about their child’s growth window, that degree of precision is not a small detail. It is the difference between acting on reliable data and acting on an approximation.
Reading the Report: What Bone Age Results Actually Mean
When you receive your child’s bone age report, the core finding will be a number, expressed in years and sometimes months, that represents where your child’s bones fall on the developmental spectrum. Here is how to interpret the three possible findings.
Bone Age Is Matched to Chronological Age
If your child’s bone age closely matches their actual birthday age, within about one year, their skeletal development is proceeding on a typical timeline. Their growth plates are maturing at the expected rate, and their remaining height potential aligns with standard growth projections for their age and gender.
This does not automatically mean there is no concern. If a child is significantly shorter than their peers despite a normal bone age, that points toward a different set of considerations, such as growth hormone output, nutritional factors, or genetic influences on adult height.
Bone Age Is Behind Chronological Age (Delayed Bone Age)
A bone age that is younger than the calendar age by more than one year is generally considered good news from a height-potential standpoint. This is the classic “late bloomer” pattern. A 13-year-old boy with a bone age of 11, for example, has two extra years of growth potential compared to a peer whose ages are matched.
His growth plates are still in an earlier stage of maturity, meaning the factory is not only still running but still has a long production window ahead. These children often feel frustrated in the short term because they appear shorter than their peers, but many of them catch up significantly and sometimes surpass their classmates in final adult height.
However, a delayed bone age is not a guarantee of becoming a late bloomer or reaching a tall adult height. It is a snapshot in time, not a fixed destiny. That said, a significantly delayed bone age is also worth monitoring carefully. One pattern that families and clinicians sometimes overlook is that bone age can accelerate and catch up to chronological age as a child’s body approaches puberty, and this acceleration does not always come with a proportional surge in height. In other words, the extra growth window that once appeared wide open can quietly narrow faster than expected, without the child visibly shooting up to match it. This is precisely why a single bone age result, even a reassuring one, should never be the last data point in the conversation.
Beyond the question of acceleration, a significantly delayed bone age is also worth evaluating for underlying causes. It can sometimes indicate constitutional growth delay or, in less common cases, an underlying hormonal issue such as growth hormone insufficiency or thyroid dysfunction. A comprehensive evaluation, including IGF-1 blood levels and growth velocity tracking, helps distinguish between a healthy late bloomer and a child whose growth needs additional support. Serial monitoring, meaning repeat bone age assessments every six to twelve months, is essential for any child with a delayed bone age. Watching how the bone age moves over time tells a far more complete story than any single result ever could.
🔍 For more on this distinction, read our related guide: Constitutional Delay of Growth and Puberty (Coming soon)
Bone Age Is Ahead of Chronological Age (Advanced Bone Age)
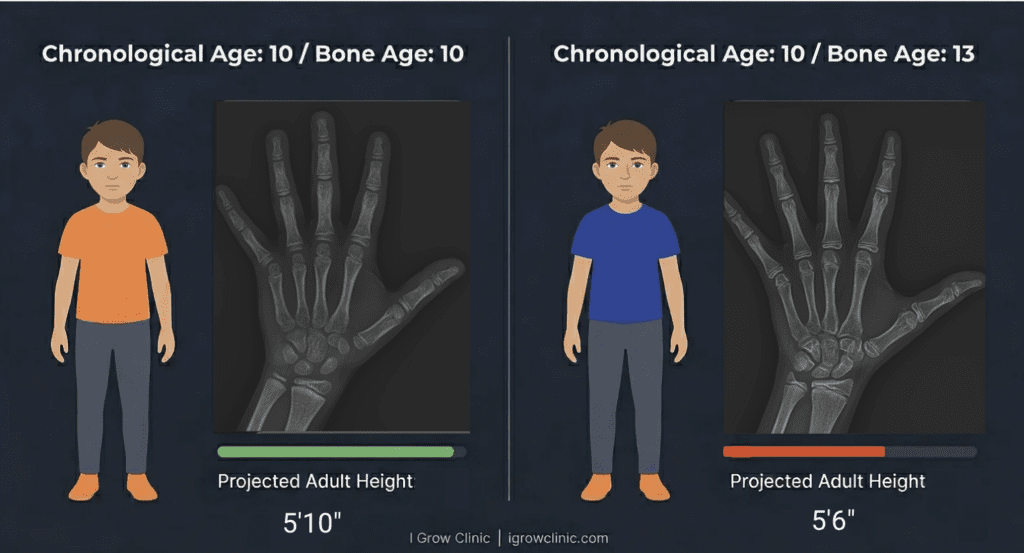
This is the finding that most concerns parents, and rightly so. A bone age that is more than one year ahead of the calendar age means the growth plates are maturing on an accelerated schedule. The most common driver of this acceleration is early puberty, a condition in which sex hormones rise earlier than expected and act as a fast-forward signal to the skeletal system.
Here is the critical insight that many families miss: a child with an advanced bone age may look like they are growing well right now. They may even be the tallest in their class. But if their growth plates fuse at age 13 or 14 while their peers continue growing until 16 or 17, they will end up shorter as adults than their early growth suggested.
This is what we call the “Tall Child Paradox,” and it is one of the most important concepts for parents to understand. Early height does not guarantee adult height. The rate at which the biological clock is ticking matters far more.
🔍 For a deeper explanation of this pattern, read: Bone Age vs. Chronological Age: Is Your Child’s Biological Clock Ticking Too Fast?.
What the X-Ray Cannot Tell You on Its Own
A bone age result is a powerful data point, but it is never the whole picture. Here is what requires additional clinical evaluation beyond the image itself.
- Growth velocity: How fast your child has been growing over the past six to twelve months tells us whether the plates are still actively producing. A child with an advanced bone age who is still growing rapidly is in a very different position than one whose growth rate has already slowed.
- Puberty stage: The Tanner staging system maps physical puberty milestones to expected growth windows. Knowing which stage your child is in puts the bone age result in the right perspective.
- IGF-1 and other lab values: Insulin-like Growth Factor 1 is a blood marker that reflects growth hormone activity. Low IGF-1 in the context of short stature or slow growth velocity may indicate that the growth plates are not receiving adequate hormonal stimulation even if they are still open.
- Predicted adult height: Using the bone age result alongside the child’s current height and growth charts, a trained clinician can calculate a predicted adult height. This estimate is far more meaningful than comparing the child to their peers right now.
🔍 For a comprehensive look at what happens as growth plates approach closure, including the physical signs you can observe at home, read: How Do You Know If Growth Plates Are Closed? 3 Key Signs Parents Often Miss.
What Happens After an Advanced Bone Age Result
If your child’s bone age is significantly ahead of their chronological age, the next step is not panic. It is action. Here is what a well-structured clinical response looks like.
Step 1: Establish the Cause
The most common driver of advanced bone age in otherwise healthy children is early puberty. However, other factors including childhood obesity, certain adrenal gland conditions, and specific genetic syndromes can also accelerate skeletal maturity. Identifying the root cause is the essential first step.
Step 2: Calculate Remaining Growth Potential
Using the bone age result and current height, we calculate how much height potential remains and what the likely adult height will be if no intervention occurs. This gives families a clear, data-based picture of what is at stake rather than a vague sense of concern.
Step 3: Discuss Whether Intervention Is Appropriate
In some cases, lifestyle optimization, nutritional support, sleep improvements, and close monitoring are sufficient. In other cases, especially when bone age is significantly advanced and puberty has arrived early, medical intervention may be appropriate to slow the rate of skeletal maturation and extend the growth window. This is a conversation that should happen with detailed clinical data on the table, not based on a hunch or a single measurement.
🔍 For families exploring this question, our pillar guide provides foundational context: What Age Do Growth Plates Close?.
A Word to the Parent Reading This Late at Night
I know what it feels like to sit with a report that you cannot fully interpret, to search the same terms again and again hoping for a clearer answer. That is not anxiety. That is love doing its best with incomplete information.
What I want you to know is that a bone age result, even an advanced one, is not a closed door. It is a data point that tells us where your child is today and how much runway may remain. The families who do best are the ones who find out early and act while the window is still open, not the ones who waited until everything was already decided.
Every milestone matters. Every centimeter is worth understanding. And you deserve to have that conversation with someone who takes the time to actually explain what the numbers mean for your child.
Your Next Step: Precision Beats Guesswork
Whether your child’s bone age result came back exactly as expected or significantly different from their calendar age, the most important thing you can do now is pair that result with a complete clinical picture.
At I Grow Clinic, we use AI-enhanced bone age analysis alongside growth velocity data, puberty staging, and lab values to give you a complete and accurate picture of your child’s remaining growth potential. We offer in-person consultations at our Fullerton, California clinic and telehealth appointments for families in California, New York, Texas, Washington, and Florida. We have many families from outside these states who fly in for an in-person consultation, and we are honored to be the destination they choose when the answer truly matters. The window may still be open. Let’s find out together.
FAQ: What Parents Ask About Growth Plate X-Ray Results
1. Does a bone age X-ray expose my child to harmful levels of radiation?
No. The radiation dose from a bone age X-ray of the hand is extremely low, comparable to or less than the natural background radiation a person receives over a few days of normal life. It is far lower than a chest X-ray and considerably less than a dental X-ray. The clinical value of the information gained far outweighs the minimal radiation exposure.
2. My child’s bone age is advanced. Does that mean they definitely won’t grow anymore?
Not necessarily. It means the growth window may be narrowing, but how much time remains depends on how advanced the bone age is and which growth plates are still active. A comprehensive evaluation that includes current height, growth velocity, and puberty stage is needed to estimate remaining potential accurately.
3. Can bone age be improved or slowed down?
While maturation that has already occurred cannot be reversed, the rate of future maturation can sometimes be influenced. Addressing the underlying cause of advancement, whether that is early puberty, excess weight, or another factor, can help slow the pace. In appropriate clinical cases, medical options exist to extend the growth window.
4. Should I request a bone age X-ray from my regular pediatrician?
You can ask your pediatrician to order one, and many will if there is a documented concern about growth patterns. If your pediatrician is not familiar with advanced bone age interpretation or prefers a wait-and-see approach, a specialist consultation at a clinic focused specifically on pediatric growth can provide a much more detailed and actionable analysis of the results.
5. How often should bone age be reassessed?
For children who are being actively monitored or supported for advanced bone age, a follow-up X-ray is typically done every six to twelve months. This allows the clinical team to track the rate of maturation over time and adjust the care plan accordingly. For children whose first result was normal and whose growth is on track, less frequent reassessment may be appropriate.
Explore More from I Grow Clinic
What Age Do Growth Plates Close?
Bone Age vs. Chronological Age: Is Your Child’s Biological Clock Ticking Too Fast?
How Do You Know If Growth Plates Are Closed? 3 Key Signs Parents Often Miss
This content is for educational purposes only and is not a substitute for professional medical advice. Please consult a qualified specialist for your child’s specific situation.