When “He’s Just a Late Bloomer” Is No Longer Enough
Picture your son at lunch in the school cafeteria, standing a full shoulder shorter than every kid at the table. He doesn’t say anything about it. But you notice. You have been noticing for two years. And every time you bring it up at his annual checkup, you leave with the same answer.
“His doctor keeps telling us he’s fine. But fine compared to what? He hasn’t grown more than an inch in the past year, and his friends are shooting up.”
At I Grow Clinic, we hear versions of these exact concerns every week. Most of the families who reach us have already been told, more than once, that their child is “fine.” And in many cases, technically, that is true. No thyroid disorder. No chronic illness. No measurable growth hormone deficiency.
Their diagnosis is idiopathic short stature, which simply means significantly shorter than peers, with no identifiable medical cause. And for these families, that “normal” label often becomes a dead end. No diagnosis means no referral, no conversation, and no plan. Growth hormone therapy exists precisely for children in this situation, but most parents never hear about it until the window is already closing.
Today, I want to walk you through what the science actually says, what the treatment actually involves, and how we at I Grow Clinic help families make this decision with clarity, data, and confidence.
Meet Sunjo Chung, FNP at I Grow Clinic
Hello, I am Sunjo Chung, FNP at I Grow Clinic in Fullerton, California. We have helped more than 2,500 children and their families navigate the complexities of short stature. We serve families both in person at our Southern California clinic and through specialized telehealth services across CA, NY, WA, FL, and TX. Our approach is always the same: move past the “wait and see” cycle, give you honest answers grounded in science, and make sure you never find out too late.
Why Families Trust I Grow Clinic
| Patients Guided | Over 2,500 children with precision growth strategies |
| Retention Rate | 95% treatment retention rate |
| Care Model | Meticulous 1:1 personalized management with AI-driven bone age analysis |
| Medical Director | Dr. Choi, Board Certified by ABPMR, 20+ years of experience |
| Rating | 5-Star Google Rating with numerous family testimonials |
| Telehealth | Available in CA, NY, WA, FL, and TX |
What Is Idiopathic Short Stature?
The word “idiopathic” simply means the cause is unknown. A child with idiopathic short stature (ISS) is significantly shorter than their peers, typically standing more than 2 standard deviations below the average height for their age and sex. Yet standard lab work comes back normal. There is no growth hormone deficiency on stimulation testing. No chronic illness, no genetic syndrome, no nutritional gap.
They are, by every standard measure, healthy. They are simply short.
This is exactly where many families get stuck. Not because something is wrong, but because without a clear diagnosis to point to, the medical system rarely offers a next step.
The U.S. Food and Drug Administration approved growth hormone therapy specifically for ISS in 2003, recognizing that the absence of a diagnosable cause does not mean the absence of opportunity to support a child’s growth potential. This approval opened an important door, but it also raised a question that every family in this situation deserves a clear answer to: is growth hormone therapy actually the right choice for my child?
The honest answer is: it depends. And the single most important variable is time.
The Factor Most Doctors Do Not Mention: The Growth Window
When families come to us after years of “wait and see,” the first thing we do is not order labs. We look at the growth window.
Every child has a biological clock ticking inside their bones. Growth plates, the cartilage zones at the ends of the long bones, are where new bone is produced and where height is added. During childhood and early puberty, these plates are active and open. As puberty progresses, sex hormones signal these plates to gradually harden and fuse. Once fusion is complete, no amount of growth hormone, nutrition or therapy can add height to that bone. The factory has closed.
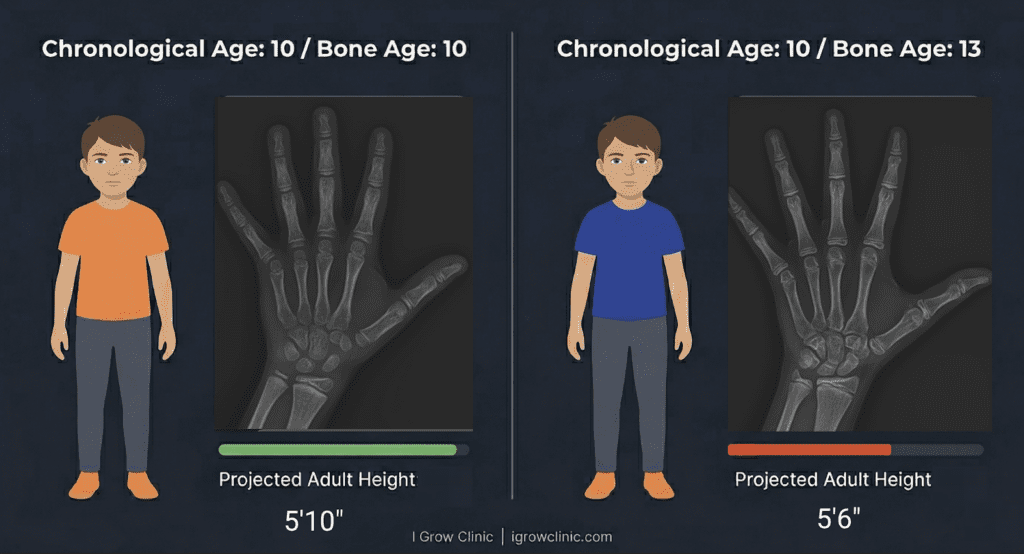
This is why a child’s bone age, or skeletal age, matters far more than the number of candles on their birthday cake. A 12-year-old with a bone age of 10 has meaningful runway left. A 12-year-old with a bone age of 14 may have a window that is already nearly closed, even if they feel and look young.
At I Grow Clinic, we use AI-enhanced bone age analysis that goes beyond a standard radiologist reading, comparing your child’s growth plate imagery against thousands of reference data points with a precision that a traditional visual estimate simply cannot match. The difference is not minor. It is the difference between a roadmap and a rough guess.
🔍To understand how bone age is measured and what the results actually mean, read our foundational guide: Bone Age vs. Chronological Age: Is Your Child’s Biological Clock Ticking Too Fast?
Does Growth Hormone Therapy Actually Work?
This is the question families ask most, and it deserves a direct, evidence-based answer.
Yes. When started at the right time, with the right patient, growth hormone therapy produces real, measurable gains in height.
Before puberty, most children grow approximately 1.6 to 2.4 inches per year on their own. With growth hormone support, that rate commonly increases to 3 to 4 inches per year. Children who begin treatment before puberty see the greatest impact on their final adult height.
During puberty, the math shifts. Children in puberty often show larger year-over-year height gains on growth hormone, but the improvement in predicted adult height accumulates more slowly compared to pre-pubertal children. This is because puberty hormones simultaneously accelerate bone maturation, shortening the remaining window even as height inches upward.
But that does not mean puberty is too late. Many of our patients are already in puberty when they start, and they still see meaningful gains. The window may be narrower, but as long as the growth plates are open, there is still opportunity worth acting on.
The takeaway is clear: earlier is better, but later is not over.
Who Can Benefit from Growth Hormone Therapy?
One of the most important things that sets I Grow Clinic apart is our belief that growth hormone therapy is not just for the child with a diagnosis. Rather than letting an insurance code define who deserves a conversation, we look at the whole picture: how fast your child is growing, how much of the window remains, and what their final adult height is likely to be without intervention. That complete picture, not a narrow eligibility checklist, is what drives every recommendation we make.
In conventional medical settings, GH therapy is discussed almost entirely within the framework of insurance-defined categories: growth hormone deficiency, idiopathic short stature below a specific percentile cutoff, or a recognized genetic syndrome. If a child does not fit one of those narrow boxes, the conversation typically ends there.
We see it differently.
Even if your child does not meet the strict insurance definitions for medical necessity, he or she may still be an excellent candidate for growth hormone support to reach a more optimal adult height. The window is either open or it is not, and that is what matters most.
Is Growth Hormone Therapy Safe?
This is the question that carries the most emotional weight, and it deserves a thorough answer.
Growth hormone therapy has been used in children for over 40 years and studied in millions of patients worldwide. When prescribed at appropriate, weight-based doses and monitored carefully by an experienced physician, it is considered very safe.
The cancer question: Growth hormone promotes cellular growth across the body. This means that in a child who already has an active cancer diagnosis, GH could theoretically stimulate existing cells. For this reason, children with a current or recent cancer diagnosis are not candidates for GH therapy. However, for healthy children with no history of cancer, decades of post-market surveillance data do not show an increased risk of developing cancer from GH therapy used at therapeutic doses.
🔍For a deeper look at this topic, read: Does Growth Hormone Therapy Cause Cancer?
The diabetes question: Growth hormone plays a natural role in blood sugar regulation, helping prevent glucose from dropping too low. When supplemental GH is added, this effect can become slightly amplified in the short term. Under careful lab monitoring and weight-appropriate dosing, the risk of developing diabetes is extremely low, close to zero, in healthy children without pre-existing metabolic concerns.
The puberty question: This is one of the most common misconceptions we address. Growth hormone does not trigger or accelerate puberty. Puberty begins when the body’s own sex hormones rise, and those hormones then stimulate the body’s natural GH to produce the pubertal growth spurt. The reverse pathway does not operate. In fact, many of our pre-pubertal patients have been on GH therapy for two to three years and have not yet entered puberty.
Natural GH production: Some parents worry that supplemental growth hormone will cause the body to reduce its own production. Under responsible, physiologic dosing and regular monitoring, this effect is clinically insignificant. The goal is always to support the body, never to override it.
At I Grow Clinic, every child’s dosage is adjusted based on growth rate, bone age, and lab values at regular intervals. Nothing is set and forgotten.
🔍For a comprehensive look at what the research says about long-term safety, read: Growth Hormone Side Effects and Safety: A Specialist Answers
What Does Treatment Actually Look Like?
For families who have never encountered growth hormone therapy before, the practical reality of what treatment involves is often the missing piece.
Growth hormone is administered through daily subcutaneous injections, typically given in the evening before sleep, when the body’s natural GH pulse is already active. The needle itself is very short and fine, placed just beneath the skin into the fat layer, making the process far more manageable than most families expect.
At regular follow-up visits, we assess growth rate, review bone age X-rays, and adjust dosage as needed to ensure the treatment remains appropriate and effective. We also monitor IGF-1 levels through regular blood work, as this marker gives us a reliable window into how effectively growth hormone is working at the cellular level.
🔍To understand what IGF-1 is and why it matters, read: IGF-1 Levels and Height Growth
These appointments are available both in person at our Fullerton clinic and through telehealth for families in CA, NY, WA, FL, and TX.
The length of treatment varies based on when it begins and how much of the growth window remains open. Some families choose to continue through puberty. Others reach a point where the bone age data tells us the window has meaningfully narrowed.
The decision to start, continue, or stop is always made together, with the data in front of us and the family’s values and goals at the center of the conversation.
The Heart of This Decision
If you have read this far, you already know something most parents don’t.
You are not here because you want to change your child. You are here because you love them and you are paying close enough attention to notice something that other people keep telling you not to worry about.
That instinct matters. Too many families came to us at 14 or 15 only to discover that the window we could have used together had already quietly closed.
Growth hormone therapy is not a guarantee of inches. It is a thoughtful, evidence-based decision we make together, only after a thorough review of your child’s growth velocity, bone age, pubertal timing, and predicted adult height. When the data supports it and the timing is right, it can make a meaningful difference. And we will never recommend it when it does not.
What I can promise is this: you will never leave a consultation without knowing exactly what the window looks like and what your options are while it remains open.
A Promise from I Grow Clinic
Your child’s potential is not a number on a growth chart. It is a story that is still being written. Our job is to make sure you have the data, the guidance, and the time to write the best possible version of it.
Whether you visit us in Fullerton or connect with us through telehealth from New York, Texas, Washington, or Florida, the conversation starts the same way: with your child’s unique biology, your family’s goals, and an honest look at what the window shows.
Do not let the clock run out on “wait and see.” Schedule your Precision Growth Consultation today.

FAQ: What Parents Ask Most About Growth Hormone Therapy
1. Does my child have to be officially “short” to be seen at I Grow Clinic?
No. We work with children across a wide range of heights and situations. What matters most is whether the growth window is still open and whether treatment aligns with your family’s goals. We evaluate each child individually, not against a checklist.
2. How is idiopathic short stature different from growth hormone deficiency?
Growth hormone deficiency means the pituitary gland is not producing enough growth hormone, which is confirmed through stimulation testing. Idiopathic short stature means a child is significantly short with no identifiable cause, and standard GH testing comes back normal. Both situations can benefit from growth hormone support, but the diagnostic pathway differs. At I Grow Clinic, we evaluate both presentations and tailor our recommendations to the individual child’s biology and goals.
3. At what age should we start the conversation?
The earlier the better, not because younger children automatically need treatment, but because early evaluation gives us the most complete picture of the growth window before any meaningful portion of it has closed. We see children as young as six. An evaluation at eight or nine, even if treatment is not yet indicated, gives the clinical team the baseline data needed to make a timely, well-informed decision later.
4. How will we know if treatment is working?
We measure growth rate at every follow-up visit and compare it to pre-treatment velocity. A positive response typically appears within the first six months as a meaningful acceleration in height gain. We also monitor bone age regularly to ensure the treatment is supporting growth without disproportionately accelerating skeletal maturation.
5. What happens if we decide not to treat?
For some children, particularly those with a bone age that closely matches their chronological age, careful monitoring without immediate treatment is genuinely appropriate. For others, especially those whose bone age is advancing ahead of schedule, every month of waiting is a month of the window closing. The goal of our evaluation is to tell you precisely which situation your child is in, so that the decision to wait or to act is grounded in data, not in hope.
Explore More
What Age Do Growth Plates Close?
Bone Age vs. Chronological Age: Is Your Child’s Biological Clock Ticking Too Fast?